The CREXONT Difference
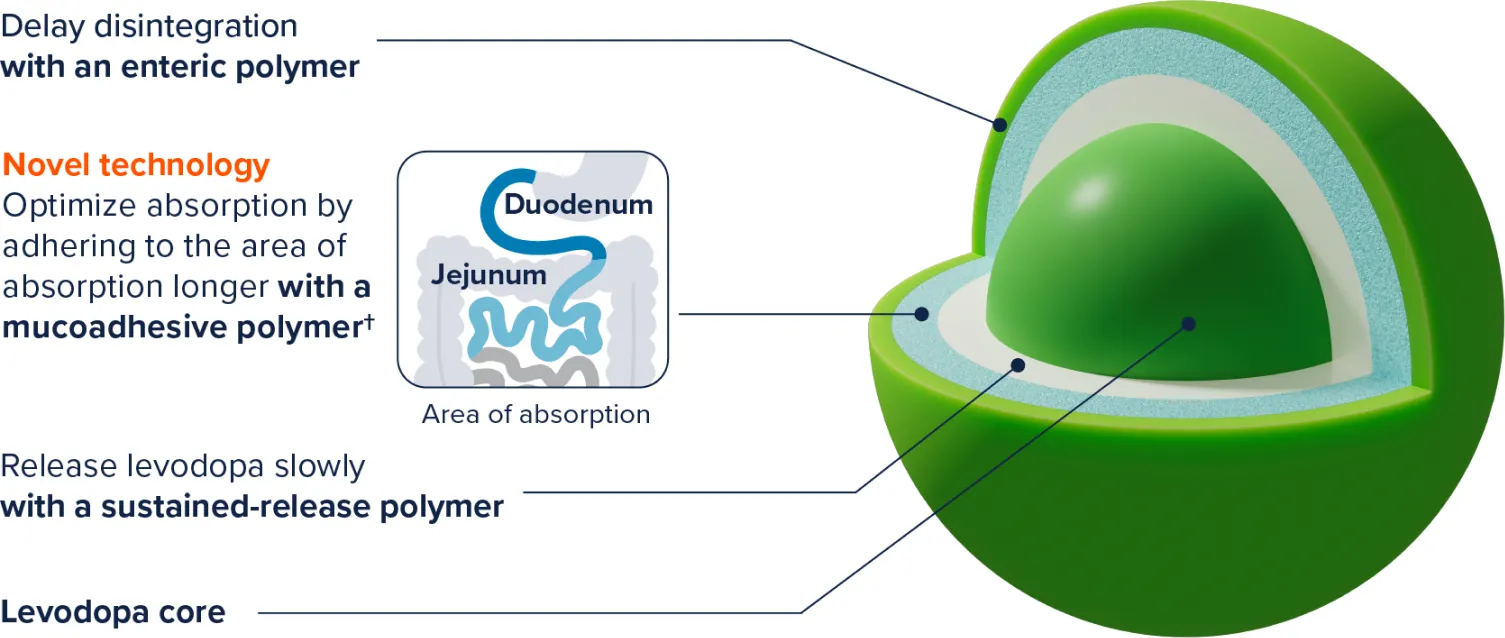
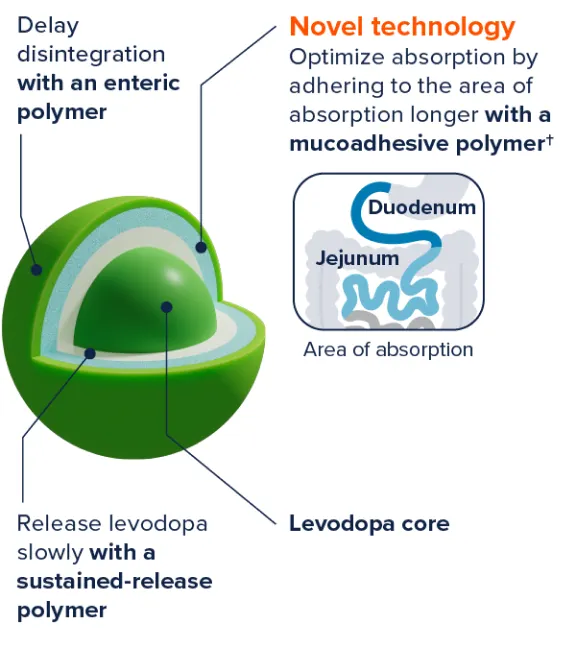
CREXONT features a novel ER technology1
| IR CD/LD | RYTARY® | CREXONT® | |
|---|---|---|---|
| Immediate-release (IR) component | |||
| Extended-release (ER) component | |||
| Mucoadhesive polymer technology |


| IR CD/LD | RYTARY® | CREXONT® | |
|---|---|---|---|
| Immediate-release (IR) component | |||
| Extended-release (ER) component | |||
| Mucoadhesive polymer technology |