Explore ELEVATE-PD Phase 4 Interim Results
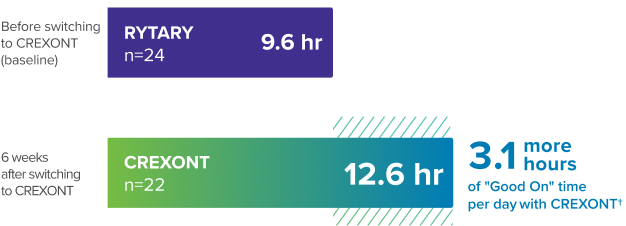
In ELEVATE-PD interim results (n=111), CREXONT increased “Good On” time per day by 3.3 hours after switching from other oral LD therapies1*†
Results from an ongoing open-label Phase 4 study of patients with PD who switched to CREXONT and continued treatment for 6 weeks were consistent with FDA-approved labeling
ELEVATE-PD: an ongoing Phase 4 study
Expanding clinical understanding to reflect real-world practice
- Efficacy measured from the start of dose conversion
- Response rates of patients switching from RYTARY (carbidopa and levodopa) extended-release capsules
- Results from an open-label study designed to mirror real-world use
*Other oral LD therapies included IR CD/LD (with or without a bedtime dose of CR CD/LD), IR CD/LD plus a COMT inhibitor, or RYTARY.1
†“Good On” time was defined as “On” time without troublesome dyskinesia. The mean difference from baseline was 3.3 more hours of “Good On” time per day.1,2
CD/LD=carbidopa/levodopa; COMT=catechol-O-methyltransferase; CR=controlled-release; IR=immediate-release; LD=levodopa.
Study design
ELEVATE-PD: An ongoing open-label study designed to evaluate the real-world efficacy and safety of CREXONT1
ELEVATE-PD study design*
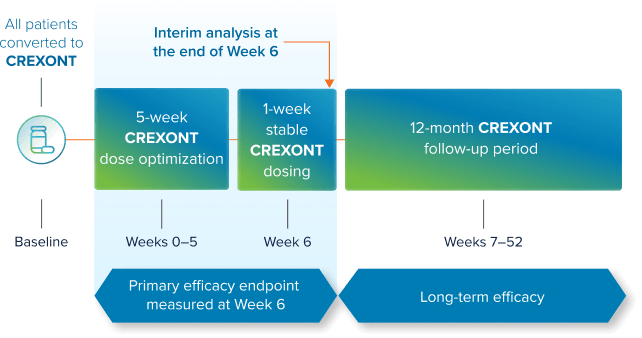
- Baseline efficacy measures were assessed before switching to CREXONT using a PD diary 3 days prior to dose conversion
- Change in efficacy was measured from baseline to Week 6 of treatment with CREXONT
- The study included patients who were previously treated with IR CD/LD, IR CD/LD plus a COMT inhibitor, or RYTARY
- Long-term (12-month) efficacy and safety results will be evaluated in this study
*CREXONT was evaluated in the Phase 4, open-label, single-arm ELEVATE-PD study over the course of 6 weeks in patients switching from IR CD/LD (with or without a bedtime dose of CR CD/LD), IR CD/LD and a COMT inhibitor, or RYTARY.1
CD/LD=carbidopa/levodopa; COMT=catechol-O-methyltransferase; CR=controlled-release; IR=immediate-release; LD=levodopa; PD=Parkinson’s disease.
Overview of the interim analysis
Early assessment of interim study results1
-
Planned interim analysis:
Predefined interim analysis of an ongoing, open-label Phase 4 study evaluating CREXONT under real-world conditions. -
Patient population:
111 of the planned ~220 patients, representing approximately half of the total study population, with outcomes assessed at 6 weeks of treatment.- Select inclusion criteria included a stable regimen of oral CD/LD, ≥20 MDS-UPDRS Part III score (“Off” state), and an average of ≥2.5 cumulative hours per day of waking “Off” time
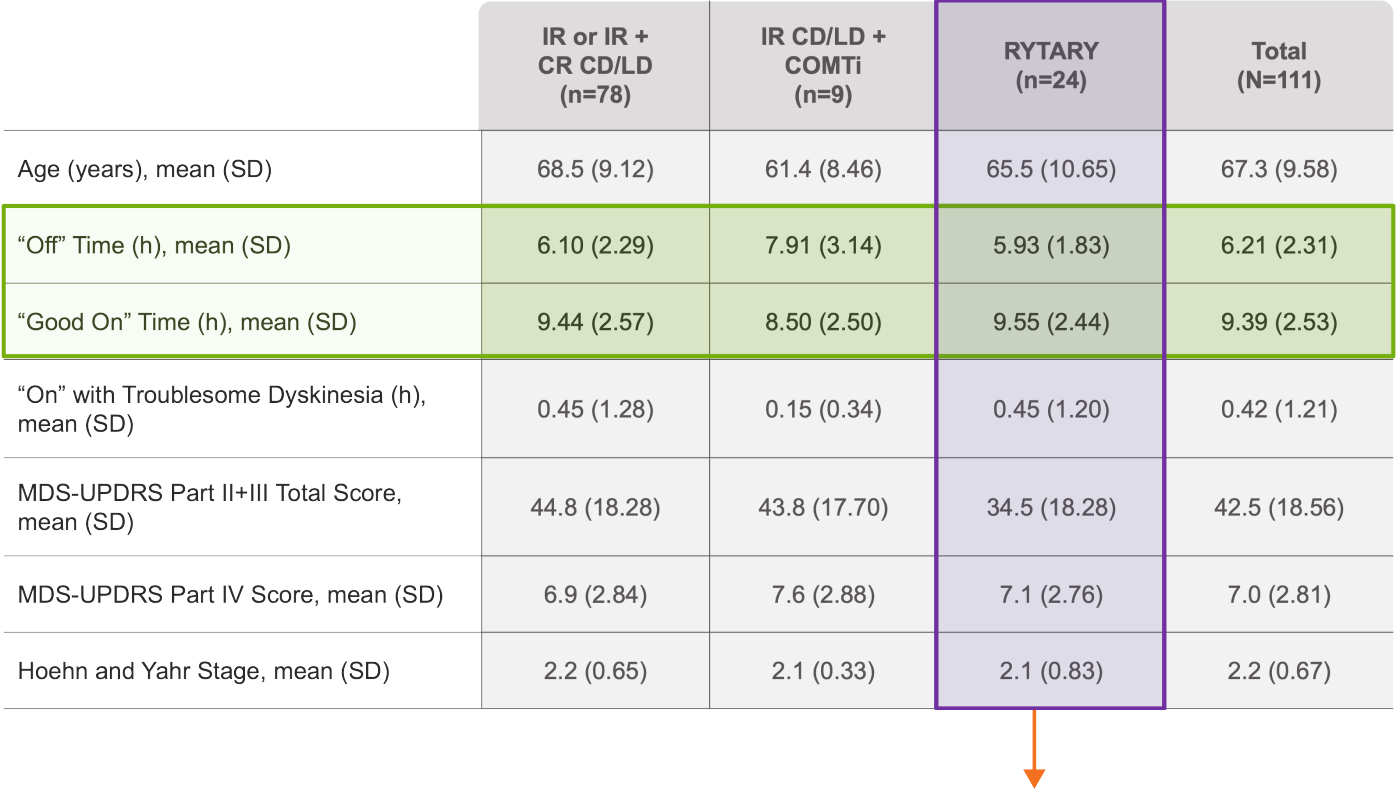 Patients previously treated with RYTARY were included in ELEVATE-PD
Patients previously treated with RYTARY were included in ELEVATE-PD -
Future analyses:
Analyses of additional patients and long-term follow-up will continue as planned throughout the 12-month study period.
Primary & secondary endpoints
CREXONT increased “Good On” time per day by 3.3 hours after switching from other oral LD therapies1*†
“Good On” time per day1
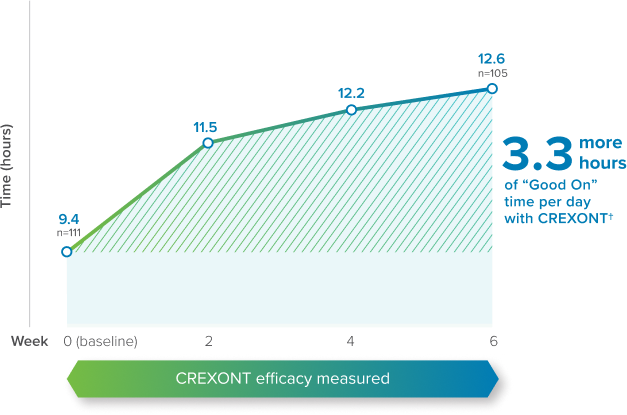
- Patients who switched to CREXONT from other oral LD therapies* experienced an improvement in “Good On” time of 3.3 hours per day (from 9.4 hours to 12.6 hours), on average
- Secondary endpoint results: Patients who switched to CREXONT from other oral LD therapies* experienced a decrease in “Off” time of 3.1 hours per day (from 6.2 hours to 3.1 hours), on average
- Average CREXONT dose frequency was 3 times per day at Week 6
*Other oral LD therapies included IR CD/LD (with or without a bedtime dose of CR CD/LD), IR CD/LD plus a COMT inhibitor, or RYTARY.1
†3.3 more hours of “Good On” time per day was the mean difference from baseline.1
CD/LD=carbidopa/levodopa; COMT=catechol-O-methyltransferase; CR=controlled-release; IR=immediate-release; LD=levodopa; PD=Parkinson’s disease.
ELEVATE-PD: Phase 4 interim subgroup analysis
Subgroup analysis showed increased “Good On” time per day regardless of prior oral LD therapy1*†
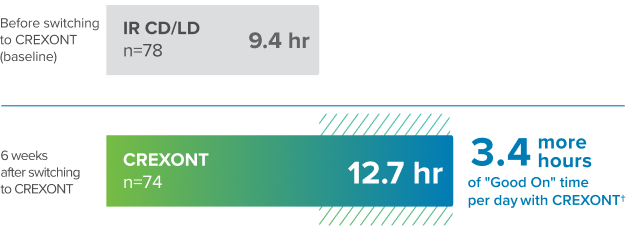
“Good On” time per day before and after switching to CREXONT from IR CD/LD1‡
“Good On” time per day before and after switching to CREXONT from RYTARY
Increase in “Good On” time and decrease in “Off” time after switching to CREXONT from other oral LD therapies1*
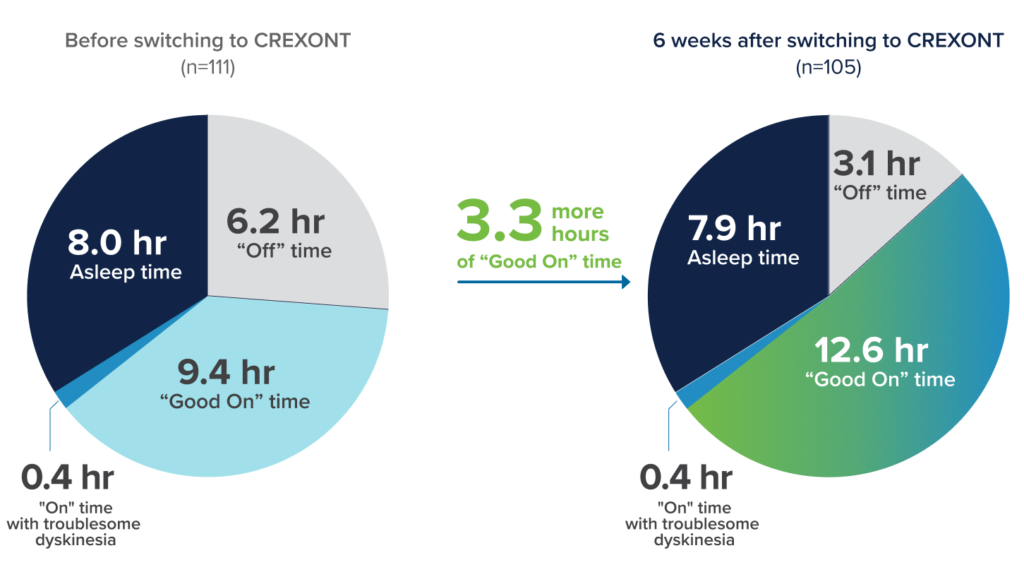
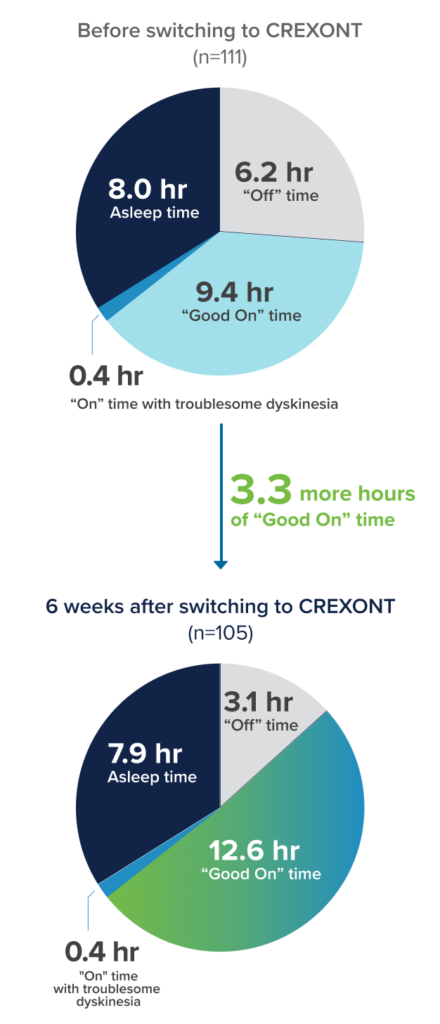
- Patients who switched to CREXONT from other oral LD therapies* experienced an improvement in “Good On” time of 3.3 hours per day (from 9.4 hours to 12.6 hours), on average1
- The increase in “Good On” time occurred with a decrease in “Off” time
* Other oral LD therapies included IR CD/LD (with or without a bedtime dose of CR CD/LD), IR CD/LD plus a COMT inhibitor, or RYTARY.1
† “Good On” time per day as measured was the mean difference from baseline.1
‡ Patients switching from IR CD/LD included patients on IR CD/LD alone or on IR CD/LD with a single bedtime dose of CR CD/LD.1
CD/LD=carbidopa/levodopa; COMT=catechol-O-methyltransferase; CR=controlled-release; Hr=hours;
IR=immediate-release; LD=levodopa.
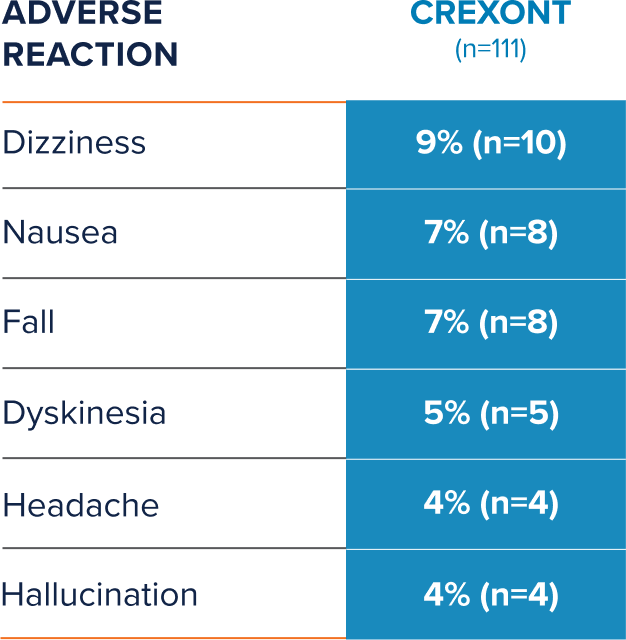
Phase 4 interim safety profile
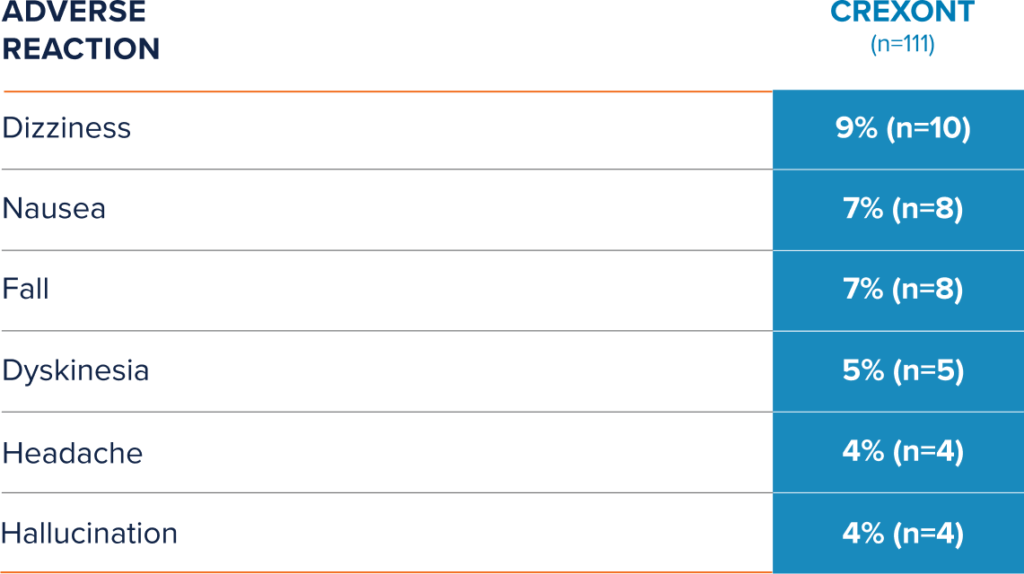
CREXONT safety profile in ELEVATE-PD interim results1
Review Safety Results from RISE-PD Pivotal Trial
IMPORTANT SAFETY INFORMATION
Indications and Usage
CREXONT® (carbidopa and levodopa) extended-release capsules for oral use is indicated for the treatment of Parkinson’s disease, post-encephalitic parkinsonism, and parkinsonism that may follow carbon monoxide intoxication or manganese intoxication in adults.
Dosage and Administration
- Evaluate vitamin B6 levels before and during treatment with carbidopa/levodopa therapies.
- Levodopa-naïve patients: Starting dose is 35 mg carbidopa/140 mg levodopa taken orally twice daily for the first three days; thereafter, dosage may be increased gradually as needed
- For patients converting to CREXONT from immediate-release carbidopa/levodopa, dosages are not substitutable on a 1:1 basis. See full prescribing information Section 2.2 for instructions
- For patients converting from Rytary® (carbidopa and levodopa) extended-release capsules, initiate CREXONT on an approximately 1:1 mg basis using the levodopa component for conversion
- CREXONT may be taken up to four times daily. The maximum recommended daily dosage is 525 mg carbidopa/2100 mg levodopa
- CREXONT may be taken with or without food. CREXONT capsules should not be chewed, divided or crushed. For patients who have difficulty swallowing, the capsule can be opened and the entire contents can be sprinkled on a small amount of applesauce and consumed immediately. Patients should not store the drug/food mixture for future use
- CREXONT should not be taken with alcohol
Contraindications
Nonselective MAO inhibitors.
Warnings and Precautions
- CREXONT may cause falling asleep during activities of daily living, somnolence or dizziness. Patients should avoid activities that require alertness such as driving and operating machinery until they know how CREXONT affects them
- It is important to avoid sudden discontinuation or rapid dose reduction to reduce the risk of withdrawal symptoms such as high fever or confusion. Patients who are discontinuing CREXONT should taper off with healthcare provider guidance
- Consider dose reductions or stopping CREXONT in patients with hallucinations or impulse control disorders (e.g., gambling, sexual urges, or uncontrolled spending)
- Consider dose reduction in patients with dyskinesia
- Treatment with carbidopa/levodopa, including CREXONT, may contribute to reduced vitamin B6 levels. Seizures associated with vitamin B6 deficiency have been reported. Seizures were refractory to traditional anti-seizure medications and were only resolved after vitamin B6 administration. Supplement with vitamin B6 as necessary
- Other symptoms of vitamin B6 deficiency may occur, including depression, confusion, cheilosis, glossitis, dermatitis, anemia, and/or neuropathy. Supplement with vitamin B6 as necessary
- Patients with a major psychotic disorder should not be treated with CREXONT
- Monitor patients with a history of cardiovascular disease for cardiac function
- Monitor patients with a history of peptic ulcer for upper GI hemorrhage
- Monitor patients with glaucoma for increased intraocular pressure
Adverse Reactions
The most common adverse reactions (incidence ≥ 3% and greater than immediate-release CD/LD) are nausea and anxiety.
Drug Interactions
Iron salts and dopamine D2 antagonists, including metoclopramide, may reduce the effectiveness of CREXONT.
Use in Specific Populations
Pregnancy: Based on animal data, CREXONT may cause fetal harm. There are no adequate data on the developmental risk associated with the use of CREXONT in pregnant women.
Breastfeeding: The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for CREXONT.
Geriatric patients: There were no differences in safety outcomes between patients less than 65 years of age, 65-75 years of age, or 75 years and older.
To report SUSPECTED ADVERSE REACTIONS, contact Amneal Global Patient Safety at 1‑877‑835‑5472, or FDA at 1‑800‑FDA‑1088 or www.fda.gov/medwatch
Please see full Prescribing Information for CREXONT.
Content is for guidance only. Please use clinical judgment when prescribing CREXONT. Dosage is individualized for each patient.
